
What Is Physician Credentialing: A 2026 Guide
TL;DR:
- Physician credentialing verifies a doctor’s education, licensure, and professional history to ensure safe practice. It takes 3 to 5 months initially and requires ongoing updates every 2 to 3 years. Proper credentialing safeguards patient safety, ensures legal compliance, and enables physicians to bill insurance networks.
Physician credentialing is defined as the formal process of verifying a doctor’s education, training, licensure, and professional history to confirm eligibility to practice medicine safely and legally. Every hospital, insurance network, and medical group in the United States requires this process before a physician can treat patients, bill insurers, or hold clinical privileges. The physician credentialing process typically takes 3–5 months for initial approval and repeats every 2–3 years to keep records current. Understanding what credentialing involves, why it matters, and how it differs from related processes like privileging gives healthcare administrators a clear picture of one of medicine’s most critical compliance functions.
What are the main steps in the physician credentialing process?
Physician credentialing follows a structured sequence that moves from document collection through independent verification and final committee review. Each step serves a specific purpose, and skipping or rushing any one of them creates legal and operational risk for the entire organization.

1. Application and document collection
The process starts when a physician submits a formal application along with supporting documents. Core credentialing documents include medical school diplomas, state medical licenses, DEA certificates, board certification records, and proof of malpractice insurance. Incomplete applications are the single most common reason credentialing stalls before it even begins.
2. Primary source verification
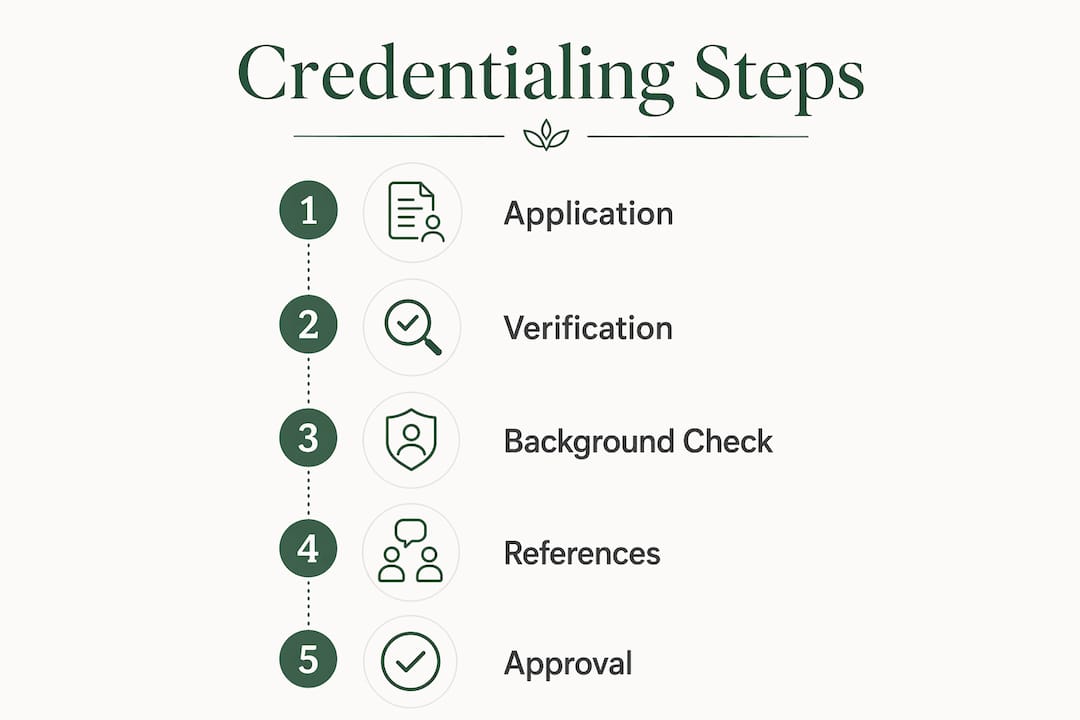
Primary source verification (PSV) is the step where a credentialing body contacts the original issuing institution directly, not the physician, to confirm each credential. Licensing boards, medical schools, and residency programs all receive direct inquiries. This step removes the possibility of falsified documents passing through undetected.
3. Background and malpractice history review
Credentialing bodies review a physician’s malpractice claims history, any disciplinary actions from state medical boards, and federal exclusion databases such as the OIG List of Excluded Individuals and Entities. A history of repeated malpractice claims does not automatically disqualify a physician, but it triggers deeper review. Transparency here is non-negotiable.
4. Peer references
Most credentialing applications require three to five professional references from physicians who have directly observed the applicant’s clinical work. These references assess clinical competence, ethical conduct, and professional character. A credentialing committee weighs these alongside objective records to form a complete clinical assessment.
5. Committee review and approval
A medical staff credentials committee reviews the completed file and votes on approval. Hospitals and health systems typically convene these committees monthly, which means a file that misses one meeting cycle waits another 30 days. Final approval grants the physician the right to proceed to privileging and insurance enrollment.
Pro Tip: The American Medical Association advises that gaps in work or education history longer than 30 days require written explanation. Leaving these gaps unexplained is the most preventable cause of credentialing delays.
How long does physician credentialing take?
Initial credentialing takes 3–5 months on average, though that range shifts based on several factors within and outside the physician’s control. Recredentialing, the renewal cycle every 2–3 years, moves faster because the baseline file already exists, but it still requires active management.
Several factors determine where a specific case lands within that range:
- History complexity. A physician with training at multiple institutions, international credentials, or prior disciplinary actions requires more verification contacts and longer review cycles.
- Primary source responsiveness. Medical schools and licensing boards vary widely in how quickly they respond to verification requests. Some institutions take weeks; others take days.
- Application completeness. A file submitted with missing documents or unexplained gaps goes back to the physician for corrections, adding weeks to the timeline.
- Committee meeting schedules. Monthly committee cycles mean a complete file submitted one day after a meeting waits a full month for the next review.
- Use of Credentialing Verification Organizations. Electronic Credentialing Verification Organizations (CVOs) coordinate multi-agency verification and can reduce turnaround time compared to manual outreach.
The practical implication is clear: a physician who submits a complete, well-documented application through a CVO and follows up proactively with primary sources will credential faster than one who waits passively.
Pro Tip: Providers should maintain current documentation at all times, not just when a credentialing cycle begins. Keeping licenses, certifications, and malpractice coverage updated year-round cuts weeks off the next application.
Why is physician credentialing vital for patient safety?
Credentialing protects patients by creating a verified record that every physician practicing in a facility or network has met defined standards of education, training, and conduct. Without this verification layer, a hospital or medical group has no reliable way to confirm that the person treating patients is qualified to do so.
The patient perspective reinforces this point directly. 93% of patients say board certification is a priority when choosing a physician. That number reflects a genuine public expectation that the doctors they see have been independently evaluated, not just hired. Credentialing is the mechanism that makes that expectation a reality.
The financial and legal stakes are equally significant. Without completed credentialing, a provider cannot bill Medicare or Medicaid, cannot admit patients to a hospital, and cannot receive reimbursement from payer networks regardless of clinical skill. A single uncredentialed physician practicing in a facility creates billing fraud exposure and potential liability for the entire organization.
Board certification, a key component of credentialing review, carries its own clinical weight. The American Board of Medical Specialties documents that board certification correlates with better patient outcomes, including reduced mortality and lower readmission rates. Credentialing is not a bureaucratic checkbox. It is a direct link between physician qualifications and the quality of care patients receive.
“Credentialing professionals see their role as a critical safety function bridging compliance and physician practice, not merely administrative.” — NAMSS Gateway
The role of physician credentials extends beyond individual patient encounters. When a medical group can demonstrate that every provider on staff has been fully credentialed, it builds institutional trust with payers, regulators, and the community it serves.
What is the difference between credentialing, privileging, and insurance enrollment?
Many physicians and administrators treat these three terms as interchangeable. They are not. Each represents a distinct process with different legal implications, and all three must be completed before a physician can practice and bill independently.
| Process | Definition | Who controls it | Key outcome |
|---|---|---|---|
| Credentialing | Verification of qualifications, education, licensure, and history | Hospital medical staff office or payer | Confirms the physician meets minimum standards |
| Privileging | Authorization to perform specific clinical procedures at a facility | Hospital credentials committee | Defines the exact scope of clinical practice |
| Insurance enrollment | Registration with a payer network to receive reimbursement | Insurance company or CVO | Enables billing and payment for services |
Credentialing comes first. It establishes that a physician is qualified in general terms. Privileging builds on that foundation by specifying what procedures the physician may perform at a particular facility. A neurosurgeon credentialed at a community hospital may not automatically receive privileges for every procedure they perform at an academic medical center. Each facility evaluates scope independently.
Insurance enrollment runs parallel to or after credentialing. A physician who is credentialed and privileged but not enrolled with a payer cannot bill or be reimbursed for services rendered to that payer’s members. The American Academy of Pediatrics notes that falsification or omissions in any of these applications can result in loss of medical license, removal from hospital staff, and exclusion from federal health programs. The consequences apply across all three processes, not just credentialing alone.
Understanding this distinction matters for administrators scheduling a new physician’s start date. Credentialing approval does not mean the physician is ready to see patients and generate revenue. All three processes must reach completion first.
Key Takeaways
Physician credentialing is the foundational verification process that confirms a physician’s qualifications, protects patient safety, and enables legal and financial participation in healthcare delivery.
| Point | Details |
|---|---|
| Credentialing verifies qualifications | Primary source verification confirms education, licensure, and malpractice history directly with issuing institutions. |
| Timeline is 3–5 months initially | Application completeness and primary source responsiveness are the two biggest factors affecting speed. |
| Patient safety depends on it | 93% of patients prioritize board certification, and credentialing is the process that validates those credentials. |
| Three processes must all complete | Credentialing, privileging, and insurance enrollment are separate steps; all three are required before a physician can practice and bill. |
| Accuracy is non-negotiable | Falsification or omissions in credentialing applications can result in license loss and exclusion from Medicare and Medicaid. |
Credentialing as a regulatory audit, not a formality
I have seen administrators treat credentialing as a paperwork exercise that sits between hiring and the first day of work. That framing causes real problems. Credentialing is a regulatory audit of a physician’s entire professional history, and it deserves the same preparation you would give a Joint Commission survey or a CMS review.
The most common mistake I observe is physicians submitting applications without reviewing their own National Practitioner Data Bank (NPDB) report first. Surprises in that report, such as a malpractice settlement they forgot to disclose, create delays that could have been avoided with 30 minutes of preparation. The healthcare credentials process rewards physicians who treat it proactively.
The second mistake is assuming that approval at one institution transfers to another. It does not. Each hospital and each payer runs its own independent review. A physician joining a new group in 2026 should expect to restart the full cycle, even if they were credentialed at a similar facility six months earlier.
My practical advice: build a credentialing file that you maintain continuously, not reactively. Keep digital copies of every license, certification, and malpractice policy. Log renewal dates in a calendar with 90-day advance alerts. When a credentialing body contacts your primary sources, follow up with those sources yourself to confirm they responded. Proactive communication with credentialing coordinators cuts weeks off the process and signals the kind of professional character that committees notice.
Credentialing in 2026 is also evolving. More payers and hospital systems are adopting electronic CVOs and shared credentialing databases to reduce redundant verification. Physicians who maintain clean, current digital records will move through these systems faster than those who still rely on paper files.
— Krunal
Gardenstatemedicalgroup and the physicians behind your care
Gardenstatemedicalgroup serves patients in North Bergen and Secaucus, New Jersey, with a team of fully credentialed physicians across primary care, cardiopulmonary services, radiology, and specialized health programs. Every provider on staff has completed the full credentialing and privileging process, so you can be confident in the qualifications of the care team you see.
Whether you are a patient seeking a trusted primary care physician or a healthcare administrator looking to understand the standards behind the providers you work with, Gardenstatemedicalgroup’s primary care services reflect the same commitment to verified, high-quality care that credentialing is designed to protect. The group also offers chronic care management programs for patients managing ongoing conditions, all delivered by physicians whose credentials have been independently verified. Contact Gardenstatemedicalgroup directly to schedule an appointment or learn more about the specialties available at either location.
FAQ
What is physician credentialing in simple terms?
Physician credentialing is the process of verifying a doctor’s education, training, licenses, and professional history before they are allowed to practice at a hospital or join an insurance network. It confirms that the physician meets established standards for safe, legal medical practice.
How often does a physician need to be recredentialed?
Recredentialing occurs every 2–3 years at most hospitals and payer networks. The cycle ensures that a physician’s licenses, certifications, and malpractice coverage remain current and that no new disciplinary actions have occurred since the last review.
Can a physician practice without completing credentialing?
No. Without completed credentialing, a physician cannot hold hospital privileges, bill Medicare or Medicaid, or receive reimbursement from payer networks. Practicing without proper credentialing creates significant legal and financial liability for both the physician and the institution.
What documents are required for physician credentialing?
Standard required documents include a medical school diploma, state medical license, DEA certificate, board certification records, proof of malpractice insurance, and professional references. Any gaps in employment or training history longer than 30 days also require a written explanation.
What happens if a physician provides false information during credentialing?
Falsification or omissions in a credentialing application can result in loss of medical license, removal from hospital medical staff, and permanent exclusion from Medicare and Medicaid programs. The American Academy of Pediatrics notes that full transparency about work and education history is a legal and professional requirement.